Full-Mouth Rehabilitation and Bite Management of Severely Worn Dentition
Released on: March 30, 2009, 8:27 am
Author: Cosmetic Dentist Virginia
Industry: Healthcare
 Introduction
Introduction
Creating a beautiful smile for a patient is extremely rewarding for the
dentist as well as for the team, and this should never be taken for granted.
We are blessed with the ability to change someone’s self esteem, confidence
and, possibly, the course of their life.
The case presented here was featured on the cover of the Spring 2008 issue
of The Journal of Cosmetic Dentistry. While it was quite challenging, I will
never forget this case,, as it changed the life of a recovering bulimia patient.
Eating disorders affect approximately seven million people in the United
States. Although I have seen the effects of bulimia on the dentition previously,
never have I witnessed it to this extent.
The patient was diagnosed with loss of vertical dimension as a direct result of
bulimia and bruxism.
Patient History
The patient, a 30-year-old female, wanted to improve her smile and to
address the constant fracturing of her teeth. Although it was difficult for her
to discuss, she told me about her history of bulimia and that after a long
struggle, she is now recovered. She was ready not only to change her smile,
but also to see what could be done about her “collapsing” face, as she put it.
She confessed that her unwillingness to smile was affecting her socially and
that she always covered her mouth when she laughed (Fig 1).
Clinical Evaluation and Diagnosis
After performing a thorough clinical examination, I noted a severely
worn dentition, widespread abfraction lesions, and multiple fractured teeth
and restorations. The palatal surfaces of the maxillary anterior teeth were
completely eroded and devoid of enamel, as is typically seen with bulimic patients (Figs 2 & 3). As expected,
the patient’s teeth were very sensitive
to temperature changes. Tooth
#5 had been extracted due to a fractured
root, and in its place was a successfully
osseointegrated implant
(Straumann USA; Andover, MA)
that had been placed one year earlier.
She had lost approximately 30%
of the length of her central incisors
due to attrition. Upon radiographic
examination, no severe decay or
pulpal pathology was evident. Periodontal
probing depths were within
normal limits.

The patient suffered from many
typical symptoms of temporomandibular
disease (TMD), such as
joint pain, severe headaches, tinnitus,
and orofacial muscle pain with
spasms.1 These symptoms were not
surprising, as craniomandibular
dysfunction is often seen with loss
of vertical dimension. She was also a
severe bruxer and said this provided
her with relief. Due to this vertical
loss, the lower third of her face was
collapsed and disproportionate. The
patient was diagnosed with loss of
vertical dimension as a direct result
of bulimia and bruxism; this was accompanied
by multiple fractured,
eroded teeth, and worn restorations. Additionally, the patient had
facial asymmetry and multiple TMD
symptoms due to craniomandibular
dysfunction.2
She tolerated the orthotic well and
felt much better with it in place.
Treatment Plan
Initially this case was overwhelming,
as there were so many factors
necessary to achieve a successful
treatment outcome. After mounting
and studying the casts, it was
obvious that the patient’s vertical
dimension had to be increased to a
proper, comfortable position, which
has been called the physiologic neuromuscular
position.3 Once this position
was determined, an orthotic
appliance would be worn to verify
that this proposed position was in
fact well tolerated and that the TMD
symptoms had decreased significantly. During the orthotic therapy
phase, this appliance would be worn
for a minimum of three months (for
a minimum of 22 hours a day), to
determine whether it would help
before any permanent alteration of
the patient’s teeth.
During this time, her condition
would be evaluated for elimination
of symptoms, proper occlusion, improvement
in facial symmetry, esthetics,
and acceptable phonetics. If
we had not seen improvements during
the orthotic phase, the first thing
we would have looked at was compliance. If it had been determined
that the patient was not wearing
the appliance as instructed, or if the
therapy had had to be extended beyond
three months (due to inconsistent
symptoms or an unstable
bite position), we would have used a fixed orthotic appliance, which
would have been fabricated to the
same vertical dimension as the removable
orthotic.4
The goal, for any clinician, is
to find a position in which the patient’s
symptoms are eliminated, or
at least decreased significantly. The
facial and dental esthetics also must
be greatly enhanced. Although there
is more than one way to find this
physiologic position, in this case I
objectively measured muscle activity
by using electromyography (EMG)
instrumentation (Myotronics-Noromed;
Kent WA). This enabled me
to locate the correct resting position
for the mandible where the muscles
are at rest, as well as the correct opening
and closing trajectory.5 During
the course of orthotic phase therapy,
which can last several months to a
year, the patient returns to verify the
bite and evaluate symptoms several
times. Once it is determined that
the patient is comfortable, facial esthetics
are improved, and the EMG
muscle activity is verified to be physiologic,
then the restoration phase
can begin.6,7

Treatment Discussion
The first step in this case was to
determine how much to increase
the patient’s vertical dimension.
Once this position was determined,
it was imperative to test and verify it;
and, most importantly, to maintain
it throughout the different phases
of treatment. The treatment phases
were as follows: Orthotic, preparation,
temporization, and cementation.
Finding the Bite
To evaluate the state of the
patient’s habitual bite position,
we had to record and evaluate
EMG readings of several muscle
groups bilaterally (K7 instrumentation,
Myotronics-Noromed). The
muscle groups measured were the
anterior and posterior temporalis
muscles, the masseters, and the
anterior digastrics. Electrodes were
placed over these muscle groups and
electromyographic recordings were
made. High EMG readings represented
a state of muscle hypertonicity
and unrest. The goal was to find
the occlusion where the muscles that
control jaw position are in a relaxed
state, and therefore are at their ideal
resting length for optimal function
and comfort.8,9
To find a more optimal bite position,
a series of diagnostic tests were
performed. These included electrosonography
to record and analyze
joint sounds, electromyography to
record and analyze muscle activity,
and computerized mandibular scanning
(CMS) to track and analyze jaw
movements. It was determined that
the patient’s habitual occlusion was
in a muscular state of hyperactivity
when at rest and in light centric occlusion
(Fig 4). In order to relax her
muscles, which were in a chronic
spasmodic state, ultra-low frequency
transcutaneous electrical neural
stimulation (TENS) was applied
using a myomonitor (Myotronics).
The myomonitor stimulates cranial
nerves V, VII, and XI to relieve hypertonicity,
restore normal blood flow,
and wash away toxic wastes such as
lactic acid. This restores the muscles
temporarily to a relaxed and normal
resting length (Fig 5). These muscles
become “deprogrammed,” and, by
measuring their pre- and post-relaxation
status, we are provided with
precise and objective comparative
data.10,11 The details of all the tests performed during the three-hour
diagnostic appointment are beyond
the scope of this article.


The position at which this patient’s
muscles were in their most
relaxed state was captured by using
a polyvinyl siloxane bite registration
material (Regisil, Dentsply Caulk;
Milford, DE). Impressions were then
taken (Aquasil Ultra, Ivoclar Vivadent;
Amherst, NY) and sent to the
laboratory with the bite to fabricate a
lower removable orthotic. Upon delivery
of this appliance, I explained
to the patient that it must be worn
a minimum of 22 hours a day. Each
follow-up visit always consisted of
45 minutes of TENS, followed by
any necessary occlusal adjustments
to the orthotic. The patient was seen
at one-, two-, three-, four-, and sixweek
intervals. She tolerated the orthotic
well and felt much better with
it in place; therefore, compliance
was not an issue.12,13
Once it was determined that the
bite was stable and that symptoms
were significantly reduced, EMG recordings
were taken again to verify
that the muscles were not hypertonic
in this new position. In this case the
EMG readings were more than satisfactory,
and the patient’s headaches
and other symptoms were reduced
significantly. Therefore, I had great
confidence as to where to restore her
occlusion.14 Her bite was opened 4
mm. The next phase of treatment
was the restorative phase.
Bite Management
(Laboratory Phase)
Much effort was spent determining
the proper physiologic position
for this patient, and much care had
to be taken in managing and maintaining
this position throughout
the course of treatment. Prior to the preparation appointment, new
impressions were taken and sent to
the laboratory, along with the actual
adjusted orthotic to mount the case.
In addition, three measurements
were provided so that the laboratory
could verify that the case was
properly mounted. These measurements
were taken with a digital Boley
gauge. The areas measured were
where the most apical areas of tooth
surface intersect with the gingiva
between teeth #8 and #25, #14 and
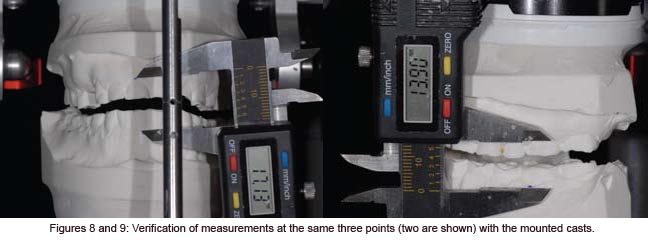
#19, and #3 and #30 (Figs 6 & 7).
In this situation, the dentist and the
laboratory must measure in the exact
same three locations throughout the
course of treatment, so as to ensure
accuracy and precision in maintaining
the new vertical (Figs 8 & 9).

Once the laboratory mounted
the casts with the adjusted orthotic
in place and the three measurements
were verified, a bite stent (Sil-Tech, Ivoclar Vivadent) was made, to
be utilized during the preparation
appointment to ensure accuracy
in maintaining the new vertical dimension.
The appliance was then
immediately returned to the patient
so that she could continue to wear
it. The laboratory also was provided
with detailed instructions concerning
the smile design, including
widths and lengths of anterior teeth,
shapes, and proportions.15

Because the patient’s maxillary
anterior teeth were short, it was determined
that crown lengthening
was necessary to support the restorations.
Therefore, the proposed
amount of hard and soft tissue removal
was relayed to the laboratory
so that they could compensate for
the change in measurement in this
area. With this information in hand,
they waxed up the 28 teeth in the
new position, taking into consideration
the hard and soft tissue reduc-tion in the anterior; and once again
verified the three measurements (Fig
10). From this wax-up, they prepared
a temporization stent made
from Sil-Tech putty and relined with
a light-body wash material (Aquasil
XLV, Dentsply Caulk). This would
be used to fabricate the 28 temporaries
after tooth preparation, with
the same vertical dimension and occlusion
as the orthotic.
Bite Management
(Preparation Phase)
Prior to the preparation appointment,
I ensured that I received everything
necessary from the laboratory.
First, I verified that the waxed-up
models were consistent with the
three measurements I had provided
to the laboratory, by measuring the
teeth in the exact same three locations.
Second, I verified that I was
satisfied with the smile design and
occlusion. As this was to be a lengthy
appointment, the clinical team met
and reviewed procedures.
After the patient was seated, I
verified the bite stent that had been
made on her unprepared, mounted
models by placing it in her mouth
and having her close down on it.
I again measured the same three
locations and verified that those
measurements were the same as
they were with the orthotic in place
(Fig 11). I was confident that all of
my numbers were accurate, so it was
time to begin preparing the teeth.
It was imperative not to lose control
of the bite at any time during the
preparation.
After anesthetizing the patient,
the first step was to perform the soft
and hard tissue crown lengthening in
the maxillary anterior region to improve
the length of her short clinical
crowns. To accomplish this, I used
an Er,Cr:YSGG hard/soft tissue laser
(Waterlase, Biolase Technologies;
Irvine, CA) and at the same time
performed a frenectomy between
the maxillary central incisors. Using
this laser provided a predictable result
and gave me a clean field within
which to work. I removed 1.2 mm
of tissue and therefore changed the
location of my uppermost point for
measurement after the crown lengthening.
I had to adjust my number
for verification from this point on,
in this area only16 (Fig 12).
It was imperative not to lose control
of the bite at any time during
the preparation. To help in maintaining
this vertical dimension, I
used the bite stent provided by the
laboratory to sequentially reline it
while I prepared one quadrant at a
time. Beginning with the upper right
quadrant, I prepared ##3-8, while
leaving #2 unprepared to provide
extra stability while I relined the bite
stent. To register the bite, I sat the
patient upright and placed a small
amount of fast-setting bite registration
material (Regisil Rigid) in the
bite stent, being careful not to overfill
it and to reline only the prepared
teeth. This was then placed in the
mouth with the patient biting into
it. While the stent was in her mouth,
the same three locations were measured
again, remembering that the
anterior area had a new measurement.
If the measurements had not
matched those taken previously it
would have been necessary to repeat
the reline, as the patient might have
been biting incorrectly or the bite
stent might not have been seated
over the teeth properly.

Once it was determined that the
measurements were correct, the
stent was removed, trimmed, and set aside for the next quadrant. The
same procedure was repeated for
the upper left quadrant, preparing
##9-14 and leaving tooth #15 unprepared.
This quadrant was then
relined the same way. After the measurements
were verified, I prepared
#2 and #15 (Fig 13). This procedure
was repeated for the bottom right
quadrant and then the bottom left.
A final check of the measurements
was made and the bite stent was set
aside to send to the laboratory along
with final impressions. For these, I
used a PVS heavy-body material and
an extra-low viscosity wash material
(Aquasil Ultra-heavy and XLV). A
symmetry bite was also taken, indicating
to the laboratory the proper
occlusal plane and midline. Photographs
of the preparations, which
showed the measurements with the
final bite stent seated and with the
symmetry bite in place, were provided
for the laboratory.
Temporization
The provisional restorations were
fabricated using the temporary stents
made from the wax-up. The stents
were filled with temporary material
(Luxatemp shade B1, Zenith/DMG;
Englewood, NJ) and placed over the
maxillary prepared teeth. After three
minutes the stent was removed, as
was a small amount of flash. This
procedure was repeated for the bottom
teeth. Once the provisionals
were in place, all three measurements
were once again verified; at
this time we evaluated esthetics and
occlusion. To properly maintain the
health of the gingival tissue during
the four-week provisional phase, the
patient was given a sonic toothbrush
(Sonicare, Philips Healthcare; Andover,
MA), as well as instructions
on how to use rubber tips to massage
her tissue. A follow-up visit was
scheduled for the next day to confirm
that the occlusion was comfortable
and that we were both satisfied
with the smile design.
Laboratory Communication
Proper communication with the
laboratory is crucial for a successful
outcome in each and every case
sent to our ceramist. In this case, it
was important to send as much information
as possible with regard
to maintenance of the patient’s vertical
dimension, as well as esthetics.
Photographs showing all three
measurements in the final bite stent,
as well as in the provisionals, were
sent to the laboratory. In addition,
retracted frontal and lateral views of
the preparations were provided, as
well as a picture showing the prepared
shade (Vita A3, Vident; Brea,
CA).17 When the laboratory received
the case, the first step was to verify
the measurements after mounting
the prepared models. This was accomplished
by using the relined bite
stent and verifying the accuracy of
the vertical dimension in the same
three locations.



For the smile design, we decided
on a “soft” look with square oval
central incisors and slightly rounded
laterals and canines, with the
lateral incisors 0.5 mm shorter than
the centrals. The requested width of
the central incisors was 8.25 mm
and the length was 10.75 mm. The
lateral incisors were approximately
10.25 mm long. Golden proportion
rules and smile design principles
were adhered to, which provided
the patient with a very soft and esthetically
pleasing smile. Our final
shade choice was OM2 body with
a cervical blend to OM3 (Vita 3D
Master shade guide), with the canines
blending from OM2 to 1M1
cervically. We selected Authentic
pressable ceramic (Jensen Indus-tries; North Haven, CT) for all anterior
teeth and bicuspids, using an
OP1+ ingot with cutback technique
and adding intense opaque modifiers
to increase vitality and a natural
appearance (Fig 14).18 All of the
molars were restored with Noritake
CZR pressable ceramic (Zahn Dental,
Henry Schein; Melville, NY) over
zirconia copings.19 The #5 implant
was restored with a custom abutment
with Creation porcelain (Jensen
Industries). Prior to the fabrication
of the restorations, the models
were mounted using the preparation
bite stent, and all the measurements
were verified by the laboratory
(Figs 15-18).
Cementation
After we received the case from
the laboratory, I checked the restorations
on the models for proper
margins and contacts, and to ensure
that the smile design had been followed.
Once all the restorations
were mounted on the models, the
three areas were measured to verify
that the laboratory maintained the
vertical dimension. Once the patient
was anesthetized, the provisional
restorations were removed. The prepared
teeth were cleaned with pumice,
followed by hydrogen peroxide
and chlorhexidine (Consepsis, Ultradent;
South Jordan, UT). Each
restoration was tried on with water
and inspected individually. Contacts
and margins were examined, as was
the overall smile design.
Once we were satisfied with restorations,
they were cleaned with 37%
phosphoric acid, rinsed, dried, and
set aside. The molars were cemented
first using Multilink (Ivoclar Vivadent),
a self-etching universal resin
cement, with the inside of the restorations
coated with the metal/zirconia
primer (Ivoclar Vivadent). Then
all of the remaining upper teeth
except #5 were etched with 37%
phosphoric acid and rinsed, after
which a wetting agent was applied
(Super Seal, Phoenix Dental; Fenton,
MI).20 Then the bonding agent
(Excite, Ivoclar Vivadent) was placed
on the teeth according to manufacturer’s
directions and light-cured.
The restorations, which had previously
been etched with hydrofluoric
acid, were coated with Silane primer
(Kerr; Orange, CA). The luting resin
used for cementation was Variolink
Veneer +2 (Ivoclar Vivadent). All
of the restorations were placed simultaneously
and spot-cured. The
excess was then removed, followed
by the final light-cure. Tooth #5
was cemented with implant cement
(Premier Dental; Plymouth Meeting,
PA).21 The same technique used
on the maxillary teeth was applied
to the lowers. Once all teeth were
cemented, the three measurements
were once again verified to confirm
maintenance of the vertical dimension
(Fig 19). The patient returned
for follow-up appointments to make
sure her bite was stable and that she
remained symptom-free.
Conclusion and Discussion
This patient’s case involved many
of the challenges we face daily in
our practices. Just a few years ago,
however, I would not have known
in which direction to take her treatment.
Perhaps I simply would have
provided her with a bruxism appliance,
while “patching up” some of
her fractured restorations and attempting
to improve her smile by
restoring some of her anterior teeth
with direct resins. These would have
failed repeatedly, causing us both
much frustration.




I conducted a series of diagnostic
tests using computerized
instrumentation, which provided me
with objective data that I was able to
use in my treatment planning.
The key point is that this patient
initially exhibited severe occlusal
disharmony and craniomandibular
dysfunction. This can be the case
in many of our patients, and much
effort should be spent in proper diagnosis
and treatment planning.22 I
did not prepare 28 teeth in one visit
and deliver them a few weeks later.
Instead, I conducted a series of diagnostic
tests using computerized instrumentation,
which provided me
with objective data that I was able
to use in my treatment planning.
Not until the patient’s new vertical
dimension position was tested for
several months did I dare touch a
single tooth with a handpiece. Once
I did, however, it was with great confidence,
because I knew in which direction
I was headed (Figs 20 & 21).
It is well accepted that there is
more than one philosophy or method
that can be utilized to arrive at
a physiologic bite position. A discussion
of these different philosophies—
whether centric relation, centric
occlusion, or neuromuscular—is
beyond the scope of this article.23 However, as responsible clinicians,
we should study the different treatment
modalities available to our
profession before making a decision
as to which one suits us. Whichever
method you apply in your practice,
the most important factor is that it
must be in your patients’ best interests.24 Before proceeding to final
restorations, it is imperative to establish
a comfortable, stable bite derived
from verifiable, objective clinical
data (Figs 22-29).
Acknowledgments
The author thanks Duckee Lee, CDT
(Protech Dental Studio, Sterling, VA),
for his passion, talent, and technical excellence
in creating the beautiful restorations
in this case. A debt of gratitude
also goes to the American Academy of
Cosmetic Dentistry for 13 years of excellent
continuing education, camaraderie,
and a remarkable credentialing
program, in which he learned during
his Accreditation journey that, “your
hand can only perform what your eyes
have been trained to see and comprehend”;
and to the Las Vegas Institute for
Advanced Dental Studies for its dedication
to postgraduate education. Finally,
thanks, appreciation, and best wishes goto Erica, the patient in this case, for her
patience, kind spirit, and courage.
References
1. Okeson JP. Management of Temporomandibular
Disorders and Occlusion (3rd ed.). St.
Louis, MO: Mosby; 1985.
2. Coy RE, Flocken JE, Adib F. Musculoskeletal
etiology and therapy of craniomandibular
pain and dysfunction. Cranio Clin
Int 1(2):163-173, 1991.
3. Jankelson RR. Neuromuscular Dental Diagnosis
and Treatment. Volume 1 (2nd ed.).
Tokyo: Ishiyaku EuroAmerica; 2005.
4. Naeije M, Hansson TL. Short-term effect of
the stabilization appliance on masticatory
muscle activity in myogenous craniomandibular
disorder patients. J Craniomand
Disord Facial Oral Pain 5:245-250, 1991.
5. Ormianer Z, Gross M. A 2-year follow-up
of mandibular posture following an increase
in occlusal vertical dimension beyond
the clinical rest position with fixed
restorations. J Oral Rehab 11:877-883,
1998.
6. Liu ZJ, Yamagata K, Ito G. Electromyographic
examination of jaw muscles in
relation to symptoms and occlusion of
patients with TMJ disorders. J Oral Rehab
26(1):33-47, 1999.
7. Neill DJ, Howell P. Computerized kinesiography
in the study of mastication
in dentate subjects. J Prosthet Dent
55(5):629-638, 1986.
8. Mongini F, Tepia-Valenta G, Conserva E.
Habitual mastication in dysfunction: A
computer-based analysis. J Prosthet Dent
1:484-494, 1989.
9. Jankelson B. Three dimensional orthodontic
diagnosis and treatment: a
neuromuscular approach. J Clin Orthod
18(9):627-636, 1984.
10. Ow RK, Carlsson GE, Jemt T. Craniomandibular
disorders and masticatory mandibular
movements. J Craniomand Disord
Facial Oral Pain 2(2):96-100, 1988.
11. George J, Boone M. A clinical study of rest
position using the kinesiograph and myomonitor.
J Prosthet Dent 41(4):456-462,
1999.
12. Konchak P, Thomas N, Lanigan D, Devon
R. Freeway space using mandibular kinesiography
and EMG before and after TENS.
Angle Orthod 58(4):343-350, 1988.
13. Balciunas BA, Stahling LM, Parente FJ.
Quantitative electromyographic response
to therapy for myo-oral facial pain: A pilot
study. J Prosthet Dent 58:366-369, 1987.
14. Isberg A, Widmalm S, Ivarsson R. Clinical,
radiographic, and electromyographic
study of patients with internal derangement
of the temporomandibular joint. Am
J Ortho 88(6)453-460, 1985.
15. Griffin JD. How to build a great relationship
with the laboratory technician:
Simplified and effective laboratory communications.
Contemp Esthet 10(7):26-34,
2006.
16. Colonna M. Crown and veneer preparations
using the Er,Cr:YSGG Waterlase hard
and soft tissue laser. Contemp Esthet Rest
Pract 10:80-86, 2002.
17. Bengel W. Mastering Dental Photography
Hanover Park, IL: Quintessence Pub.;2002.
18. Magne P, Belser U. Bonded Porcelain Restorations
in the Anterior Dentition: A Biomimetic
Approach. Hanover Park, IL: Quintessence
Pub.; 2002.
19. Ludwig K. Studies on the ultimate strength
of all-ceramic crowns. Dent Laboratory
39:647-651, 1991.
20. Kanca J. Improving bond strength through
acid etching of dentin and bonding to wet
dentin surfaces. JADA 123:35-44, 1992.
21. Garg AK. Practical Implant Dentistry (1st
ed.). Dallas, TX: Taylor Publishing; 2007.
22. Tingey EM, Buschang PH, Throckmorton
GS. Mandibular rest position: A reliable
position influenced by head support and
body posture. Am J Orthod Dentofac Orthop
120(6):614-622, 2001.
23. Pully ML, Carr S. Solving the pain puzzle:
Myofascial pain dysfunction (3rd ed.). Albuquerque,
NM: TMData Resources; 1997.
24. Shankland WE . Temporomandibular disorders:
Standard treatment options. Gen
Dent 52(4):349-355, 2004.
Contact Details: Dr. H.R. Makarita DDS,MAGD
2936 Chain Bridge Rd
Suite 200
Oakton, VA 22124
(703) 255-1150
www.fixasmile.com


